Strategies for Knock Knees
What are knock knees? There are 2 types: One is considered "structural," meaning the bones are fixed genetically, and the other is considered "postural," meaning the bones are being pulled by muscles and can be corrected.
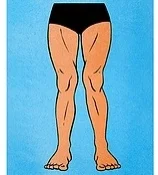
The first, structural one, is also called "genu valgum" which means the angle of the femur bone is overly accentuated and the knees touch when the feet are together and knees extended.
Let's focus on Postural Knock Knees
Postural knock knees, according to Kendall's Muscle Testing and Function are a combination of external rotation of the hip, hyperextension of the knee, and supination of the ankle.
Because the femurs are externally rotated, the knees are bending and straightening at an oblique angle, so when the knees hyperextend they "knock" each other. The supination of the ankle is a natural continuation of the lower limb being in external rotation, since supination is basically external rotation of the ankle and foot.
I also see knock knees where the femur is not in external rotation, meaning the patella is facing straight ahead. The knocking happens because the IT Bands and outer muscles of the thigh (lateral quads and hamstrings) create a kind of flexion on the transverse plane and the knees collapse inward. This almost always happens with obese people since the thighs cannot come together due to fat and the inner thighs become overly lengthened and the outer leg becomes overly tight.
In both cases the inner thighs (adductors) are long, and the lateral muscles of the leg are short.
Strategies for Postural Knock Knees:
1. Release IT Band, Lateral Quads, Lateral Hamstrings and External Rotators.
I like to use the foam roller to do this.
2. Strengthen Adductors, VMO (medial quadricep) and Medial Hamstring, and make sure to work the leg in Medial Rotation.
-Footwork in Parallel with ball between knees and bigger ball between ankles, work parallel, and make sure client puts weight in their big toe metatarsal. When doing Footwork on the Reformer (with anyone with hyperextension in the knees), have them stop before they are in their "bony end point". Have them stay in their muscles, not going into full lock out. If using a ball between the knees, have client squeeze the ball at end range to keep them "in their muscles".
-Footwork in internal rotation and "snow plow" pulses.
-Leg Springs on Reformer or Springboard/Cadillac in parallel (use ball between ankles) keeping knees soft, also work internal rotation.
-Side Splits on Reformer with light spring.
-Hamstrings on Reformer, working parallel and internal rotation.
3. Train the client to not hyperextend their knees. This is a mental challenge and is difficult to train through muscle strengthening alone. Awareness needs to be brought to standing and walking with a little "sponginess in the knees".
-Toe raises with soft knees. Have client hold onto a bar or a wall for balance, and have them soften their knees, bringing the tibia forward over the ankle joint. Do 10 toe raises not allowing the head to go up and down, but rather the knees to go forward as toes rise up. Then try single leg 10x on each side. After this exercise have the client walk around. It brings a great awareness to how the lower limb should be aligned over the ankle.