The Knee: The Stupid Joint
The knee can only flex and extend (some minor rotation movement) and is trapped between the hip and ankle, so when the knee is out of alignment most of the time it is coming from the hip or ankle.
Structural issues that cause knee pain: arthitis, shallow patella grooves, structural bow legs and knock knees, or other boney/cartilage dysfunction. Ligamental tears are a very common reason for knee for knee instability and pain. See below for ligamental tear details.
The meniscus is a C-shaped piece of tough, rubbery cartilage that acts as a shock absorber between your shinbone and thighbone. It can be torn if you suddenly twist your knee while bearing weight on it. The outside one-third of the meniscus has a rich blood supply. A tear in this "red" zone may heal on its own, or can often be repaired with surgery. ... Without nutrients from blood, tears in this "white" zone cannot heal. These complex tears are often in thin, worn cartilage. Left untreated, a meniscus tear can cause even more damage, hasten the onset of osteoarthritis, and lead to a myriad of other undesirable symptoms. Physical therapy can help you strengthen the muscles around your knee and in your legs to help stabilize and support the knee joint.
What can we do as Pilates instructors?
We can strengthen and balance the muscles around the knee joint to create more stability. And we can release overly tight muscles and fasciae that may be causing imbalance and pain.
Lateral and Patellar Knee Pain
What’s going on?
If you suffer from knee pain, particularly lateral knee pain or pain on the front of your knee, around your kneecap (patella), pain when you go down stairs, pain after you run or do any kind of impact sport, this little trick could be a lifesaver.
Patellar tracking problems, patellar subluxation of patella, patellar-femoral syndrome, IT Band syndrome all start from a similar problem. Imbalance of the quadriceps muscles, weakness in the VMO, and in the IT Band syndrome also weakness in the gluteus medius.
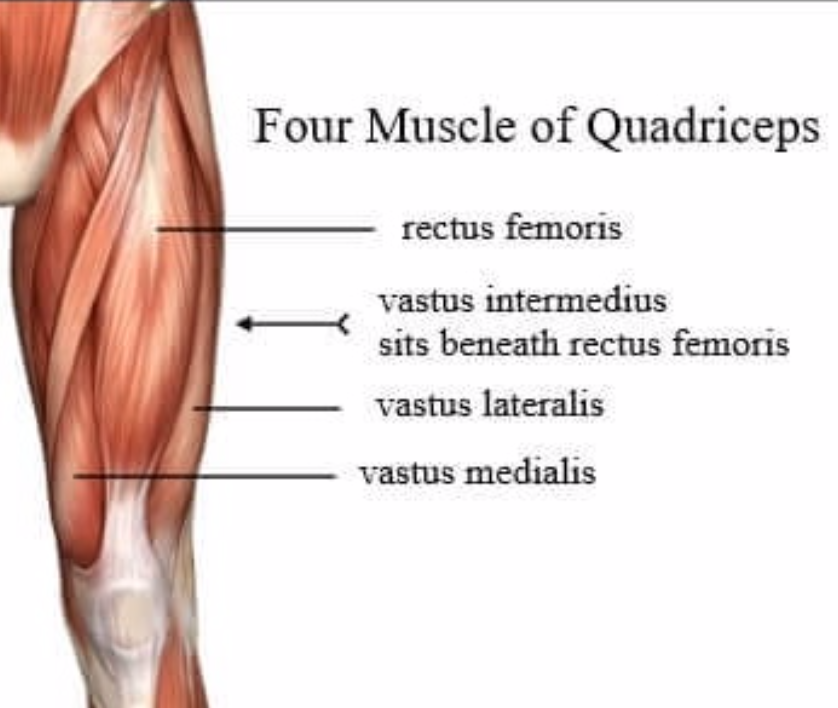
The Quads
Quadricep in Latin means 4 heads. The quads are 4 long muscles on the front of your leg that extend your knee. They all come together to form a common tendon that attaches and encompasses the knee cap (the patellar tendon). So if you have any pain in the front of your knee, or around your knee cap the culprit is probably a tight quad. Most sports overuse the quadriceps, particularly the lateral quadriceps. Running, dance, biking (if you aren't maintaining proper knee alignment pointing over the middle toe), and any high impact sports that involve the legs tend to overuse the lateral quadricep and underuse the medial quadricep. The exceptions are yoga, a good Pilates or Barre class (one that keeps the legs in parallel rather than in turn-out), swimming, ice skating, horseback riding. Knee pain, particularly lateral knee pain can be due to the imbalance of the lateral v. medial quadriceps.
VMO: Vastus Medialis Obliquus
New research shows that working the quadriceps as a group with the hip in proper alignment is more effective than focusing on the VMO in isolation.
The medial quadricep is responsible for pulling the knee cap medially at the end range of knee extension. Because many sports use the legs without fully straightening the knee, the medial quadricep may become atrophied or underutilized and basically "turn off". VMO is an acronym for the vastus medialis obliquus which is the small oblique fibers of the medial quadricep that are right above the knee cap. These fibers are particularly responsible for pulling the knee cap medially at end range of extension and maintaining proper "patellar tracking".
There are many medical terms for the imbalance of the quad group; patellar femoral syndrome, patellar tracking problems, etc. IT band syndrome is another diagnosis that also causes lateral knee pain (see below for more info about the IT band). All of these issues are due to the imbalance of the lateral and medial muscles of the knee.
Releasing the lateral quad (and the IT Band) followed by strengthening the quads, allowing all 4 quads to fire in balance.
The IT Band
The iliotibial band emerges from the Tensor Fascia Lata (TFL) in the front of the hip and the gluteus maximus in the back. It forms a long, connective tissue band that acts as a lateral stabilizer of the knee and hip. When it becomes too tight and overused it can create inflammation and pain in the lateral knee. Thus "IT Band Syndrome".
IT Band compensates for a Weak Gluteus Medius
Often the root of IT Band overuse is that the IT Band compensates for a weak gluteus medius. The gluteus medius is also a lateral stabilizer of the hip and holds the pelvis level while standing one foot, (or walking). If the gluteus medius "turns off" the IT Band does the work of the gluteus medius, but over time the IT Band will shorten and get cranky from overuse. So part of the rehabilitation process should be strengthening the gluteus medius. There are many ways to do this, but I have chosen Single Leg Bridge since it mimics gait.
When in Doubt, Roll it Out!
The more tight it is the more it will hurt. Again, like childbirth, you need to look pain straight in the eye and go into it. It’s the only way out!
Don't Cry
Rolling out your IT band can be very painful. Use a soft roller (MELT roller). I prefer these rollers for myofascial release. Start by rolling slowly up and down the lateral thigh going all the way from the top of the hip to right above the knee joint. Never roll over a bone. Next, add "cross fiber" release by rolling your thigh side to side slowly as you roll up and down. You want to do a 3-dimensional release to get at the "web-like" structure of the fascia. If you can handle it, try also bending and straightening the knee while you roll up and down. This is a killer!
There are 3 main trigger points on the IT band. In Chinese medicine, this is Gall Bladder Channel or GB for short. You want to focus on GB 31, 32, and particularly GB 33 if you have lateral knee pain and IT Band Syndrome. GB 33 will be excruciating if you are suffering from IT Band overuse. But as they say, no pain no gain. If it doesn't hurt you haven't found the trigger point!
Lateral and Patellar Knee Pain Strategy
Release/Roll out your Quads, Roll out your IT Band
Strengthen VMO and hamstrings.
Exercises
VMO End Range Knee Extension 1: Lie on your back with your knee over the roller, allowing the knee to be bent, heel on the floor. Straighten your leg, thinking of pulling the knee cap to the inside of your thigh. Flexing your foot can help. Repeat 10-20 times, twice a day.
VMO Straight-Leg Raise in Turn-Out: Turn out leg and lift up a few inches, keeping knee straight. Repeat 10-20 times, twice a day.
Footwork
Sleeper (Side Lying Footwork)
Single Leg Bridge on mat, reformer, yoga block combo
Bridge with feet together
Leg Springs first on thighs, on Reformer or Springboard/Cadillac in parallel (use ball between ankles) keeping knees soft, also work external rotation.
Squats, Side Splits on Reformer with light spring/ heavy spring
Knee Hyperextension: Its All In Your Mind!

Hyperextension of the knees happens because some people have loose ligaments and tendons around the knee joint. Often these people have looseness globally. They also may have pelvic misalignment like anterior pelvic tilt, posterior pelvic tilt or hyperextension of the hip joint (or swayback). So how can you help someone correct something that is basically a structural, genetic issue? Mind control.
A person with hyperextension of the knees needs to be conscious of how they stand and walk. They need to retrain what "straight" feels like and learn to not go to their "bony end-point". They don't get the pleasure of standing with a "locked out" knee. When the knee is locked it is very stable ligament-wise and it is easy to stand with little to no muscles needed. Keeping your knees "soft" takes some muscular work, including core work, and its hard to remember.
I have been surprised by clients’ lack of awareness of their knee hyperextension. Once you bring attention to this, clients may experience improvement in knee pain immediately. But they would never have thought to stop hyperextending. Although knee pain is not necessarily a side effect of hyperextension in the short run, in the long run, hyperextension of the knee will damage the joint. Hyperextension can also cause plantar fasciitis. Why? Read on.
What happens when the knees hyperextend?
1. Quadriceps Hypertonic: The quadricep group extends the knee, so it makes sense that when the knee is hyperextended the quads would be hypertonic.
2. Soleus Hypertonic: Because the ankle is in relative plantar flexion when the knee is hyperextended, the soleus becomes chronically shortened. The gastrocnemius, which is the other plantar flexor, is not shortened because it also crosses the knee and is lengthened over that joint, basically canceling out the shortness over the ankle. But the soleus is a one-joint muscle, so it will become chronically shortened when the knees hyperextend. And when the soleus is chronically shortened, it can cause plantar fasciitis because the Achilles tendon--which is shared by the soleus and gastrocnemius-- becomes shortened, it pulls on the fascia of the foot and creates heel pain, i.e. plantar fasciitis.
*Interesting fact: people faint when standing in knee hyperextension because the shortened soleus compresses the soleal vein and stops venus return to the heart.
*Second Interesting Fact: The soleus is sometimes called "the second heart" because it is responsible for pumping the blood back up to the heart by contracting while walking. That is why walking is so important for circulation and overall health!
3. Hamstrings long. When the knee is in a hyperextended position the hamstring is in a relative lengthened position.
Strategies for Correcting Hyperextension of the Knees:
Mental Training
As I discussed above, awareness needs to be brought to standing and walking with a little "sponginess in the knees."
Physical Training
Always correct pelvic misalignment first. Anterior Pelvic Tilt, Posterior Pelvic Tilt, and Hyperextension of the Hip Joint all can be a cause (or result) of hyperextension of the knee joint.
Exercises
Toe raises with soft knees. Have the client hold onto a bar or a wall for balance and have them soften their knees, bringing the tibia forward over the ankle joint. Do 10 toe raises, not allowing the head to go up and down, but rather the knees to go forward as toes rise up. Then try single leg 10x on each side. After this exercise, have the client walk around. It brings a great awareness to how the lower limb should be aligned over the ankle.
When doing Footwork on the Reformer have clients stop before they are at their "bony endpoint." Have them stay in their muscles and not go into full lockout. Putting a squishy ball between the knees can help feel the muscles at end range. Have client squeeze ball while extending the knee to feel the muscles stay engaged.
Leg Springs first on thighs, on Reformer or Springboard/Cadillac in parallel (use ball between ankles) keeping knees soft
Hamstrings on the Reformer. Lying prone on Long Box.
Standing Ball squeeze. With foot pointed, holding onto barre or wall for balance. Strengthens Hamstrings and plantar flexors.
Bridging with neutral pelvis. Cueing the client to send knees forward over ankle joint and pull heels toward the bottom at the top of the bridge. Strengthens Hamstrings.
Bow Legs and Internal Rotation of the Femur
Postural Bow Legs: Internal rotation of the femurs, hyperextension of the knees, pronation of the ankle
Like knock knees, there are 2 main types of "bow legs." One is s Structural Bow Legs, where the femurs are not rotated but are actually curved outward. In these cases, the knees will point straight ahead but will have space in between them when the knee is extended.
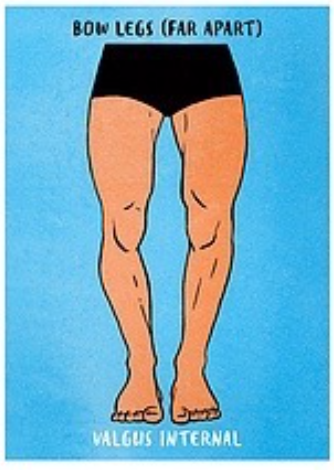
Let's talk about Postural Bow Legs, which are defined by Kendall as a combination of hyperextension of the knees, medial rotation of the femurs and pronation of the ankle. Since the femur is turned in, when the knee flexes and extends it does so at an oblique angle. When that knee is then hyperextended, the knees "bow" away from each other.
In my experience, people with this situation are usually hypermobile and are "hanging" on their joints. Often their hips are hyperextended as well.
Strategies to correct Postural Bow Legs
1. Lengthen the adductors, if tight. The adductors are the internal rotators of the hip.
Lie in a straddle with your legs against a wall, allowing gravity to open the legs.
With feet in loops on the Reformer, lie in a straddle and let the resistance pull the legs open.
2. Strengthen the external rotators of the hip.
Exercises
Clam is the best exercise for this whether it be on the mat, or with some resistance from the leg spring or theraband.
Sleeper or side lying footwork are also excellent to strengthen the outer hip muscles.
Footwork on Reformer with a Theraband around the outside of the thigh.
Squats with a Theraband around the outside of the thighs.
Leg Springs first on thighs, on Reformer or Springboard/Cadillac in parallel (use ball between ankles) keeping knees soft, also work external rotation.
Side Splits on Reformer with heavy (red) spring.
Hamstrings on Reformer, working parallel and external rotation.
3. Train the client to not hyperextend their knees.
This is a mental challenge and is difficult to train through muscle strengthening alone. Awareness needs to be brought to standing and walking with a little "sponginess in the knees."
Toe raises with soft knees. Have the client hold onto a bar or a wall for balance, and have them soften their knees, bringing the tibia forward over the ankle joint. Do 10 toe raises not allowing the head to go up and down, but rather the knees to go forward as toes rise up. Then try single leg 10x on each side. After this exercise, have the client walk around. It brings a great awareness to how the lower limb should be aligned over the ankle.
When doing Footwork on the Reformer (with anyone with hyperextension in the knees), have them stop before they are in their "bony end point". Have them stay in their muscles, not going into full lock out.
Knock Knees and External Rotation of the Femur
EXTERNAL ROTATION OF THE FEMURS, HYPEREXTENSION OF THE KNEES, SUPINATION OF THE ANKLES.

What are knock knees? There are 2 types: One is considered "structural," meaning the bones are fixed genetically, and the other is considered "postural," meaning the bones are being pulled by muscles and can be corrected. The first, structural one, is also called "genu valgum" which means the angle of the femur bone is overly accentuated and the knees touch when the feet are together and knees extended.
Let's focus on Postural Knock Knees
Postural knock knees, according to Kendall's Muscle Testing and Function are a combination of external rotation of the hip, hyperextension of the knee, and supination of the ankle.
Because the femurs are externally rotated, the knees are bending and straightening at an oblique angle, so when the knees hyperextend they "knock" each other. The supination of the ankle is a natural continuation of the lower limb being in external rotation since supination is basically external rotation of the ankle and foot.
I also see knock knees where the femur is not in external rotation, meaning the patella is facing straight ahead. The knocking happens because the IT Bands and outer muscles of the thigh (lateral quads and hamstrings) create a kind of flexion on the transverse plane and the knees collapse inward. This almost always happens with obese people since the thighs cannot come together due to fat and the inner thighs become overly lengthened and the outer leg becomes overly tight.
In both cases the inner thighs (adductors) are long, and the lateral muscles of the leg are short.
Strategies for Postural Knock Knees:
1. Release IT Band, Lateral Quads, Lateral Hamstrings, and External Rotators.
I like to use the foam roller to do this.
2. Strengthen Adductors, VMO (medial quadricep) and Medial Hamstring, and make sure to work the leg in Medial Rotation.
Exercises
Footwork in Parallel with ball between knees
Footwork in Parallel with ball between knees and bigger ball between ankles, work parallel and make sure client puts weight in their big toe metatarsal. When doing Footwork on the Reformer (with anyone with hyperextension in the knees), have them stop before they are in their "bony endpoint". Have them stay in their muscles, not going into full lockout. If using a ball between the knees, have client squeeze the ball at end range to keep them "in their muscles".
Footwork in internal rotation and "snowplow" pulses.
Leg Springs first on thighs, on Reformer or Springboard/Cadillac in parallel (use ball between ankles) keeping knees soft, also work internal rotation
Sleeper (Side Lying Footwork)
Side Splits on Reformer with light spring.
Hamstrings on Reformer, working parallel and internal rotation.
3. Train the client to not hyperextend their knees. This is a mental challenge and is difficult to train through muscle strengthening alone. Awareness needs to be brought to standing and walking with a little "sponginess in the knees".
Toe raises with soft knees. Have client hold onto a bar or a wall for balance, and have them soften their knees, bringing the tibia forward over the ankle joint. Do 10 toe raises not allowing the head to go up and down, but rather the knees to go forward as toes rise up. Then try single leg 10x on each side. After this exercise have the client walk around. It brings a great awareness to how the lower limb should be aligned over the ankle.
Knee Ligament Tears

Anterior Cruciate Ligament (ACL) Tear Strategy:
Tibia has forward movement on Femur. (Drawer test)
Release /roll out Quadriceps
Strengthen Hamstrings, Gastrocnemius:
Footwork in Parallel
Sleeper (Side Lying Footwork)
Hamstrings on Reformer
Leg Springs on Reformer and Cadillac
bridges (on roller, soft ball to increase hamstring and gastrocnemius engagement and stability),
theraband hamstring,
ball squeeze
Posterior Collateral Ligament (PCL) Tear Strategy:
Tibia has a backward movement on the femur.
Release /roll out Hamstrings
Strengthen Quadriceps,
Exercises
Footwork in Parallel with ball between knees
Leg Springs first on thighs, on Reformer or Springboard/Cadillac in parallel (use ball between ankles) keeping knees soft, also work internal rotation.
Side Splits on Reformer with light spring.
Sleeper (Side Lying Footwork)
Theraband Quadriceps, Lunging, squats
Lateral Collateral Ligament Tear Strategy:
Tibia has lateral movement on femur.
Strengthen Hip Abductors;
side leg lifts, add theraband,
squats and lateral walking squats with theraband around the outside of thighs
Footwork in Parallel with theraband around thighs.
Sleeper (Side Lying Footwork)
Leg Springs on Reformer or Springboard/Cadillac in parallel with theraband around outside.
Side Splits on Reformer with heavy spring.
Medial Collateral Ligament Tear Strategy:
Tibia has medial movement on femur.
Strengthen Hip adductors; squeeze ball between knees, ankles, squats with ball/yoga block between thighs, toe raises with ball between ankle.
Strengthen Adductors, VMO (medial quadricep) and Medial Hamstring, and make sure to work the leg in Medial Rotation.
Great General Exercises for Knee Problems
Reformer:
Footwork
Sleeper (Side Lying Footwork)
Thighs in straps, starting with knee extensions then progress to Feet in Springs
Standing Squats/Bonnie Blair speed skating/Side Splits